
Wow! We thought things may slow down for a bit after the election, but instead health policy changes seem to be happening more frequently than ever. As rates of COVID surge across the country, it is vitally important pharmacists understand these changes and how they apply to practice. By better understanding these rapid health policy changes, pharmacists will be better informed on how they can currently practice and understand where advocacy initiatives need to be focused to advance patient care in the future.
An important advocacy initiative that we have discussed on the blog is the necessity to establish a sustainable business model for the provision of pharmacist provided patient care services. Although the ability to directly bill for services is a vital goal for the profession (for more see: Why do pharmacists need provider status?), other methods have been employed to allow pharmacists to indirectly bill for their services. One of these methods is for pharmacists to bill incident to a physician for the services that they are providing. For years, there has been a lot of confusion and questions around this indirect billing method. Just last week, the Centers for Medicare & Medicaid Services (CMS) released their annual Physician Fee Schedule (PFS). Within this behemoth of a two thousand page document, it includes key information regarding pharmacist’s ability to bill incident to. This week we review incident to billing and what updates are included in the PFS.
A brief history of incident to billing for pharmacists
Pharmacists billing incident to the physician or nonphysician practitioners (NPPs) is a step in the direction toward provider status. It allows pharmacists to bill insurance companies for services that they would not normally be able to be reimbursed for because they are not recognized as healthcare providers. When this first began, it was a big breakthrough for the profession of pharmacy because it allowed pharmacists to bring in revenue to the businesses that they work for as a result of the cognitive services and medical decision making that they were providing.
Pharmacists billing incident to likely began when the American Academy of Family Physicians (AAFP) sent a letter to CMS asking for clarification if pharmacists could bill incident to physicians. In March 2014, CMS responded by confirming that pharmacists could in fact bill incident to the physician. The ability for pharmacists to bill incident to is consistent with other mid-level practitioners such as nurse practitioners and physician assistants. Although this was trumpeted as a major victory for the profession, there were major roadblocks to pharmacists in all practice settings to be able to utilize this new reimbursement methodology. One of the biggest barriers was the fact that a physician needed to be directly available to the pharmacist when providing incident to services. This was largely interpreted that the physician and pharmacist were in the same physical location and patients were being seen in person. This limited pharmacists billing incident to the physician for telehealth services and created barriers for many community pharmacists that were not practicing in the same physical location as a physician.
Another major barrier to rolling out sustainable programs where pharmacists provided services and billed incident to was regarding a belief that pharmacists could only bill the lowest level of Evaluation & Management (also known as E&M) codes. Normally, in the outpatient setting there are two sets of billing codes that physicians use as the foundation of their patient visits. These are known as E&M codes and the two sets are for new patients (99201-99205) or for established patients (99211-99215). The lower numbers of both of these codes, for example 99201 or 99211, are used for less complex patients, that require less time, and less medical decision making. These lower E/M codes are reimbursed at a lower amount than other E&M codes. As patient visits increase in complexity and time, physicians bill higher E&M codes which are reimbursed at a higher level. This helps to associate the value of services being provided by the physician with a comparable reimbursement amount. Below is a table exemplifying this from the current physician fee schedule of national payment amounts:
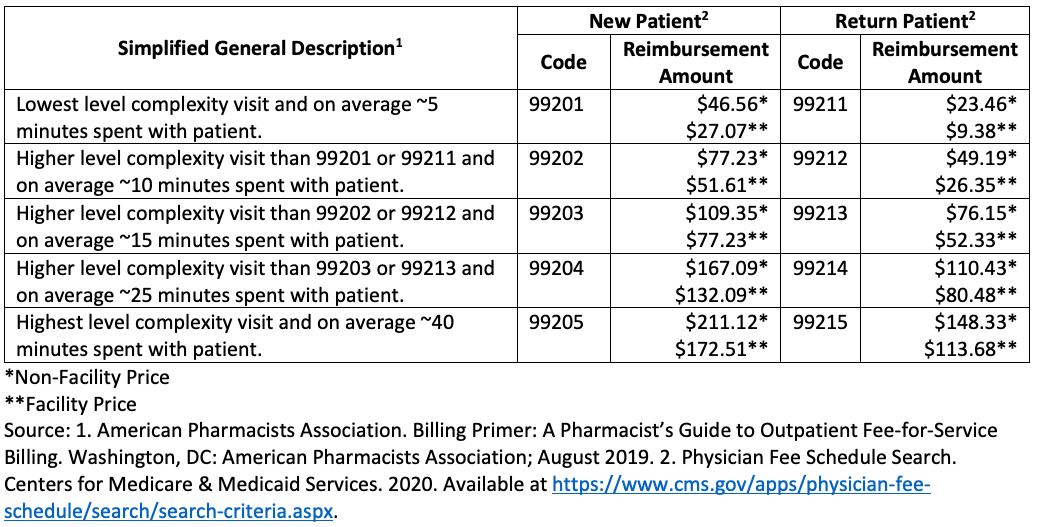
After pharmacists learned that they could bill incident to, it quickly began to spread that pharmacists were only allowed to bill the lowest level of return patient code (99211) regardless of the amount of time that a pharmacist spends with the patient or the number of interventions that are made. This information likely came from a regional Medicare Office that provided clarification that pharmacists could only bill these lowest level codes. Obviously, this is not ideal because the level of service being provided by a pharmacist would not align with the amount of reimbursement. This misalignment would create further barriers to pharmacists providing services and growing their practices.
Although information was published from Regional Medicare offices regarding pharmacists only billing the lowest level codes, there was never an explicit justification as to why this was the case. Additionally, it is not clear if all regional offices have provided this information and because of this, depending on the geographical area that pharmacists practice in, some have been billing the higher E&M codes where others have not been able to. There have even been publications (here is one from the Journal of Managed Care Pharmacy) stating that the belief that pharmacists can only bill 99211 E&M codes is simply “not true” (keep reading because this statement is in fact false). This inconsistency in policies from a national health insurance program (Medicare) is abnormal.
As the pandemic hit 2020, many of the regulations on pharmacist practicing and billing for their services have been changed. One of the key updates that we covered previously was the indication that pharmacists would continue to be able to bill incident to the physician for telehealth services. With the publication of the coming year’s PFS last week we have seen more information come out regarding pharmacists ability to bill for services incident to.
How does the PFS change incident to billing?
The PFS is an annual document that outlines the fees that Medicare will be using to pay physicians and other practitioners for the services that they provide. Additionally, CMS will take time to respond to stakeholder questions in order to provide clarification for how to appropriately utilize the PFS. The 2021 PFS can be accessed here.
Relevant to pharmacists billing incident to the physician or NPPs are pages 352-357, where stakeholders ask for clarification as to whether pharmacists can bill incident to and if they can bill all E&M codes. This question has been asked of CMS previously, however, the information included in the PFS is the most detailed response they have given to date. Included in this response is confirmation from CMS that pharmacists billing Medicare incident to physicians or NPPs can only bill the lowest level of E&M codes (99211). This is a pretty striking confirmation and may result in some pharmacists changing how they are billing for their services if they are billing Medicare incident to for higher level E&M (99202-99205; 99212-99215) codes.
Although it is not ideal that this confirmation may result in a decrease in revenue generation from some pharmacists depending on their billing practices, included in the PFS is an explanation as to why pharmacists cannot bill these higher level codes. With this explanation comes an understanding of what changes need to be advocated for in order to allow pharmacists to bill Medicare for all E&M codes incident to physicians or NPPs.
CMS explains that the reason pharmacists can only bill the lowest level E&M code is because of two definitions used in the Current Procedural Terminology (CPT) codebook. In the CPT codebook the term ‘physician or qualified health professional’ (QHP) and ‘clinical staff’ are used in descriptions as to which individuals can provide different services, such as those included in E&M codes. Specifically, included in the 2021 CPT Codebook is information that higher level E&M codes can only be provided by physicians or QHPs. These definitions are included in the table below:
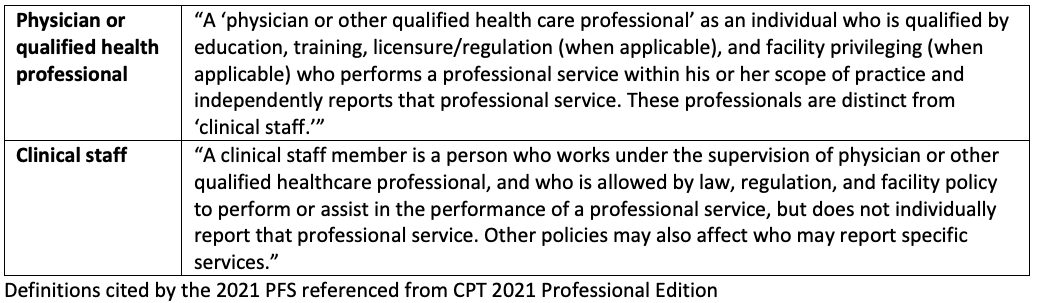
So, there is no overlap here. A QHP cannot also be ‘clinical staff’. These are mutually exclusive definitions. Included in the CPT codebook is the requirement that higher level E&M codes must be provided by a physician or QHP. Unfortunately, CMS states that they do not consider pharmacists QHPs and because of this, this is the reason pharmacists can not bill Medicare incident to for higher level E&M codes. The justification for why CMS does not consider pharmacists QHPs is that “there is no Medicare statutory benefit allowing them to enroll, bill and receive direct payment for PFS services.” The key term here is ‘direct payment’. So, even though we would be billing incident to the physician, the fact that direct payment is being used is indicative that this is still all coming back to recognizing pharmacists as providers under the Social Security Act (more information about this can be found here).
Additionally CMS states that in some settings pharmacists could be considered QHPs, however under current Medicare Law (the dreaded Social Security Act) even if a pharmacist billed Medicare, CMS says “we do not have ability to pay (or even price) services that are furnished and billed directly by pharmacists.”
What are the next steps?
So this news is not necessarily good or bad, it’s a little of both. It is bad that some pharmacists may not be able to continue to bill Medicare for higher level E&M codes, however, it is good that we now understand what must change in order to allow pharmacists to bill incident to for these higher level E&M codes. So, what needs to change? We believe there are potentially two alternate answers to this question.
The first answer would be for Medicare to recognize pharmacists as QHPs and thus allow them to bill for higher level E&M codes. Although this seems to be a simple advocacy initiative, it gets more complicated as you review the specific language that CMS used as its justification for why pharmacists are not considered QHPs. The justification that CMS uses ties back to pharmacist’s inability to directly bill for services from Medicare, which ties back to pharmacist recognition as providers in the Social Security Act, aka ‘Provider Status’. So the first answer to this question is for pharmacists to get Medicare provider status, which is not something we would recommend anyone holding their breath over…
The second alternative answer is actually outlined in the PFS as something CMS states should be considered. This is indicated when they state, “We note that new coding might be useful to specifically identify these particular models of care.” What they are suggesting here, is that the CPT codebook change the codes for higher level E&M codes to allow clinical staff (which pharmacists are frequently defined as) to bill incident to physicians or NPPs for services they have provided. This would allow CMS the ability to allow pharmacists, designated as clinical staff, to bill Medicare for higher level E&M codes incident to physicians or NPPs. Although this might seem like a simple enough ask, you are not going to like it when we tell you who owns the rights to the CPT codebook…the American Medical Association (AMA).
The AMA has expressed concern over expanded reimbursement models for pharmacists, and has even passed a resolution in their House of Delegates to this effect. Here is where you can make the difference though. Under the current model, pharmacists practicing in incident to reimbursement models are throwing away money and undervaluing their services every time they provide a level of care above a 99211 code. Expressing that revenue is being left on the table to leaders of health systems may be an enticing argument for physicians in leadership positions over health-systems or outpatient clinics. We all want the same thing, which is increasing access to high quality, effective healthcare. We know that with more revenue we can further the missions and visions of the organizations that we work for. Why leave money on the table, when a simple change by the AMA could better patient care and revenue streams for many of their members?
If you work for a health-system or outpatient clinic, we encourage you to ask this question to your administrators and physician leaders. This, along with advocating to the AMA and CMS, may open up incident to billing opportunities for pharmacists across the country, and thus enhance access to patient care.

Since E/M codes greater than 99211 can’t be used via incident to billing model, what about other CPT codes like 93793 for anticoagulation mgmt or 95251 for CGM interpretation? Are these fair game?
LikeLiked by 1 person
If Medicare recognizes pharmacists enough to code any of these codes (99211), wouldn’t that imply that pharmacists are QHP?
LikeLiked by 1 person
Unfortunately, no. Both QHP and clinical staff can bill 99211 but CMS recognizes pharmacists as clinical staff, so they are able to bill incident to at the 99211 level but are not able to bill at higher billing code levels because only QHP are allowed to.
LikeLiked by 1 person