
It’s been a while since we posted in our Provider Status Explained series because of all that has been evolving in the quickly changing world of health policy. We now want to come back to continue our discussion on one of the most important legislative priorities for the patients of pharmacists and the pharmacy profession: provider status. As a reminder, we started this series with a discussion around why pharmacists need provider status. We then began evaluating how we could achieve provider status at the federal level. Now let’s move on to the states, where things are moving much more quickly!
Medicaid
Just as we had described with the federal legislative strategy, efforts on the state level have largely revolved around the public health insurance system, Medicaid. As a refresher, the Medicaid system was established at the same time as Medicare with the signing of the 1965 Amendments to the Social Security Act. While the role of Medicare was to be a federally-funded public health insurance system primarily for the elderly, Medicaid’s role was to be a federal- and state-funded public health insurance system for those with low incomes, children, pregnant women, and people with disabilities. Where the funding comes from is vitally important in understanding how these systems are regulated. Being a completely federally-funded program, decisions on how Medicare is run are made by Congress. Alternatively, the fate of Medicaid and many of the decisions around it are largely in the hands of state lawmakers. You may jump to the conclusion that this is because funding for the programs primarily comes from the states, but this is not true, as you can see from the below map.
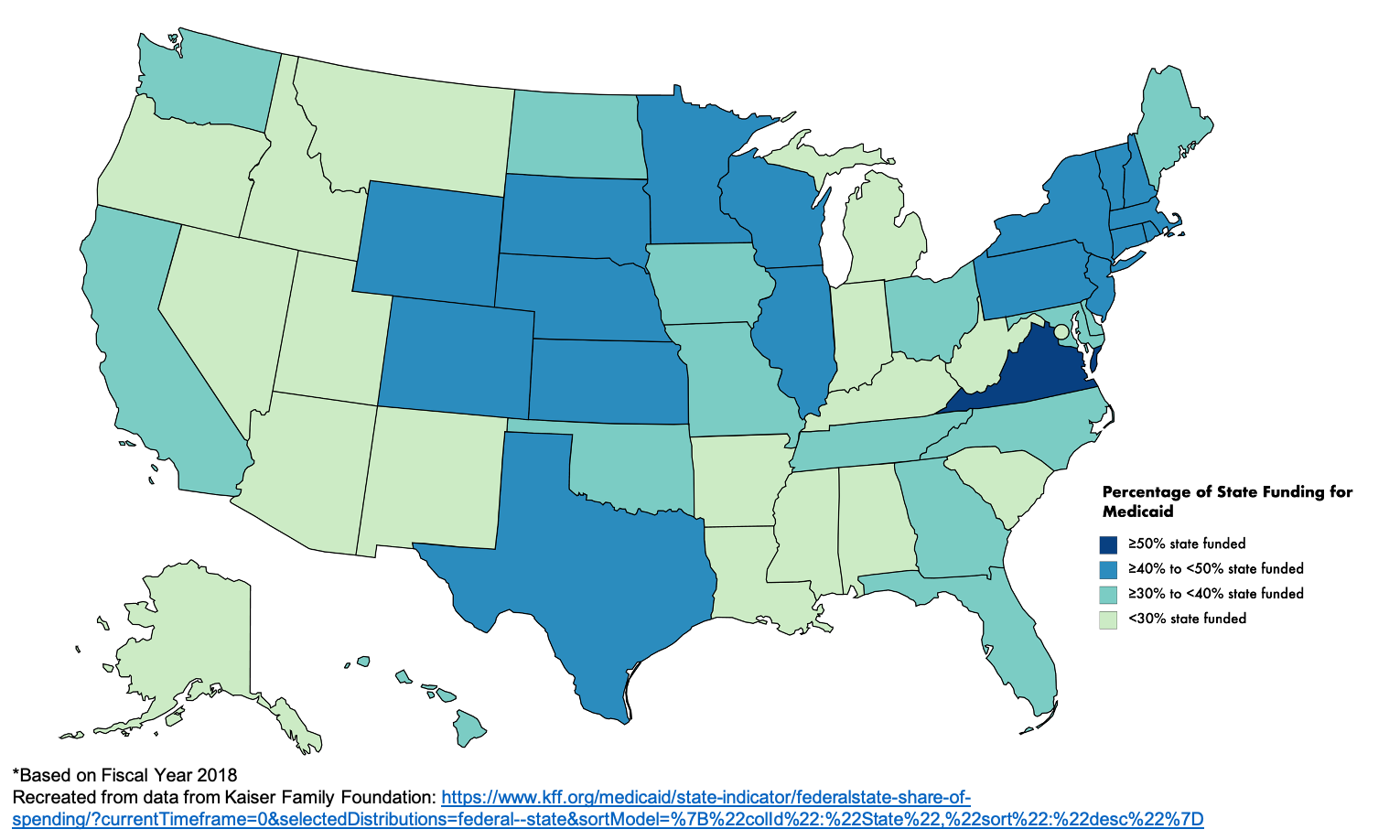
Despite the fact that only one state pays a majority of Medicaid funding (50.1% in Virginia), state lawmakers and regulators largely control the day-to-day operations of the programs, such as deciding which types of providers can enroll. This is where provider status comes in to play, and why efforts to gain provider status are focused on reaching out to your local legislators. Not as simple as the Social Security Act, where pharmacists only need to be added to the list of eligible providers, state law can be a bit messier. Some states may already recognize pharmacists as providers in some pieces of their law, or states may not recognize them at all. State-level provider status will require a consistent definition of a pharmacist as a provider through rules and laws in order to allow for them to be reimbursed by health insurance companies and Medicaid.
It is important to note, though, that the federal government is not completely out of the picture when it comes to Medicaid. They don’t just hand over up to 79% of a department’s budget without providing some oversight. Because of the complexities and opaqueness of the Centers for Medicare & Medicaid Services (CMS), as more states pass provider status, we do not know how or if CMS will react and flex their oversight muscles.
Budgetary considerations are important to understand because opponents of provider status may bring up cost implications to adding another provider to the Medicaid system. Although research, such as the Asheville Project, shows that when pharmacists provide patient care services, insurance claims eventually go down, opponents may suggest that the addition of an entire class of new providers will increase costs to the state. We are unsure of the liberty that states have with their federal funding, but if there was a place it may make sense for the feds to flex their oversight, it would be with how states specifically use their funds. And, as we know, the feds have not come around yet to the idea of the pharmacist provider. That leaves the state to deal with these potential additional costs. Due to the fact that nearly all states are required to pass a balanced budget, if a cost is added, that means either something has to go, or taxes must be raised. It is important to be prepared to address these concerns when you are advocating to state lawmakers and explain the positive therapeutic and economic value of pharmacist-provided patient care services.
The typical state story
Alright, so just like with the federal strategy, now we understand more behind how the state laws and rules have to change and basics of the complex Medicaid funding system. Let’s take a look at some states that have passed provider status and how they did it. Two of the most prominent states to pass legislation early were Washington and California. In both states, pharmacists and state associations worked effectively with their state lawmakers to pass initial legislation that recognized pharmacists as providers. However, once it was passed, they seemed to hit a wall. The laws recognized pharmacists as providers, but there was no mandate that insurance companies had to pay for the services pharmacists were providing. Many other states have also passed provider status and hit this same roadblock, ending up locked in negotiations with payors that say they are not required to pay, so why would they start?
California and Washington both went down the path of additional legislation. Going back to their state lawmakers, they were able to make the argument that the legislature’s intent with provider status legislation was not only to recognize them as providers in name, but to actually compensate pharmacists for their cognitive services. Both were able to pass additional legislation requiring payors to begin credentialing and paying pharmacists for their services. Washington’s language in this bill is generalizable, which is strong policy that can apply to new situations as the profession evolves. California’s is more specific, listing types of services that can be reimbursed, which means that every new service that pharmacists want to be paid for will require legislative or regulatory action.
And this is where most states are, hanging somewhere in between either passing provider status or passing legislation that would require reimbursement. However, one state has recently been different in their efforts to implement provider status. After passing provider status in January 2019, Ohio has had success in starting initial programs with Medicaid Managed Care Organizations (MCOs) to pay pharmacists for their cognitive services and the Medicaid Department is planning to enact rules in January 2021 to begin credentialing pharmacists as Medicaid providers. This has all happened without the passage of an additional law mandating reimbursement because of advocacy and public optics. Around the same time that provider status was passing, it was coming to light in Ohio that $244 million was unaccountable in the state budget as a result of the Pharmacy Benefit Managers (PBMs) working underneath Medicaid. There was ample media coverage of this by local news sources, which eventually led to them discussing more issues around pharmacy and provider status. We’ve explained previously on the blog the incredible importance of public advocacy. Well, all of this bad PR around PBMs and Medicaid made the MCOs in the state look around and raise their hand and say, “Actually, we want to work with the pharmacists.” As these programs continue to roll out, there could be nationwide implications and less of a need for future states to have to pass additional legislation to mandate reimbursement by payors after provider status is passed.
The question of OLP and SPA
As states have continued to pass provider status legislation, some have made the argument that an additional step needs to be taken in order for pharmacists to be enrolled as eligible providers that will be approved under CMS. Other Licensed Practitioners (OLP) are defined in rule 42 CFR 440.60 of Medicaid regulations. These are the rules that define non-physician practitioner services in Medicaid. Some have made the argument that in order for pharmacists to be enrolled as Medicaid providers, states must submit State Plan Amendments (SPA) to CMS in order to add pharmacists to the list of OLPs for the state. So far, five states have submitted SPAs and been approved under OLP rules to add pharmacists. In addition to OLP, other states have also added pharmacists as providers under Medicaid under other regulations using SPAs.
There is not much information out there regarding OLP, and it does not seem to be a requirement, as states such as Washington and Ohio do not have an approved SPA. The full necessity of OLP will need to be evaluated and clarified in the future.
Tipping of the scale
As we can see, the strategy to add pharmacists as providers under Medicaid compared to Medicare has some similarities and stark differences. Both require legislative and regulatory changes; however, states have had far more success even with incremental legislative victories in the past decade as compared to Congress. Although budgets need to be considered in both state and federal advocacy, because nearly all states have a mandate to pass a balanced budget, this adds another level of complexity.
In the past, following the passage of this legislation, there has been a need to pass additional laws to mandate health insurers to pay pharmacists. However, we have seen from recent examples that this may no longer be a requirement.
When there is not enough political will to move legislation in Congress, and as more states pass similar laws, eventually there can be a tipping of the scales and national action may be taken (as happened with the women’s suffrage movement). We should recognize how success on the state level could further influence the action of national legislation. State-level lawmakers are often more accessible than your members of Congress, so reach out and keep advocating for change on your state level. This could be the change we need to tip the scales and move forward with the federal legislative strategy for provider status!
So far, we have unpacked the “why” of provider status, and how provider status can be accomplished on the national and state level. Next on the Provider Status Explained series, we will delve into what you can do to advocate to your legislators and the public to be recognized as providers!
